Drugs are bad mmk? Well, are they? The go-to argument involves looking at drug abusers. It’s hard to say something positive about drug abuse in general. Everybody has a story to tell about some friend or family member who got into problems. But we also have people who are food abusers, i.e., who eat too much and suffer the consequences. One can also eat too little food and get into problems. Based on this analogy, then, we might question the idea that drugs are bad overall. Maybe a moderate amount of drug use is better. What does the data show? Of course, no one randomized people to take a given amount of drugs in their lives and looked at what happened, but we can look at the other phenotypes of people who never take a drug, take it sometimes, or all the time. There’s a bunch of studies that have done for various drugs. Let’s begin with a nice one:
-
White, J. W., Gale, C. R., & Batty, G. D. (2012). Intelligence quotient in childhood and the risk of illegal drug use in middle-age: the 1958 National Child Development Survey. Annals of Epidemiology, 22(9), 654-657.
Purpose High childhood IQ test scores have been associated with increased alcohol dependency and use in adult life, but the relationship between childhood IQ and illegal drug use in later life is unclear.
Methods Participants were 6713 members of the 1958 National Child Development Survey whose IQ was assessed at 11 years and had their lifetime illegal drug use measured at 42 years of age.
Results In analyses adjusted for a range of covariates, a 1 SD (15-point) increase in IQ scores was associated with an increased risk of illegal drug use in women: ever using cannabis (odds ratio [OR], 1.30; 95% confidence interval [95% CI], 1.16–1.45), cocaine (OR, 1.66; 95% CI, 1.21–2.27), amphetamines (OR, 1.50; 95% CI, 1.22–1.83), amyl nitrate (OR, 1.79; 95% CI, 1.30–2.46) and “magic mushrooms” (OR, 1.52; 95% CI, 1.18–1.98). Associations were of lower magnitude in men.
Conclusions In this cohort, high childhood IQ was related to illegal drug use in adulthood.
Looks like this:

So in this study they just looked at whether someone had tried a given drug or not. Since most people who have tried a drug are not problem users, this will mostly function as a contrast between never users vs. mostly non-problem users. The columns show the odds ratios of for intelligence. So values above 1 mean that intelligence was associated with being more likely to have tried a given drug. Not a single value is negative beyond chance level (one is negative for men, but p > .05). So overall people who have tried any drug are somewhat smarter. The associations did not go away when the authors controlled for a variety of things (the other columns). This finding was also seen in a 1980s study.
Still, it would be nicer to have a continuous measure of drug use and relate this other variables. Here’s one for alcohol:
- Degerud, E., Ystrom, E., Tambs, K., Ariansen, I., Mørland, J., Magnus, P., … & Næss, Ø. (2018). The interplay between cognitive ability, alcohol consumption, and health characteristics. Psychological medicine, 48(12), 2011-2022.
Background Higher cognitive ability is associated with favourable health characteristics. The relation between ability and alcohol consumption, and their interplay with other health characteristics, is unclear. We aimed to assess the relationship between cognitive ability and alcohol consumption and to assess whether alcohol consumption relates differently to health characteristics across strata of ability.
Methods For 63 120 Norwegian males, data on cognitive ability in early adulthood were linked to midlife data on alcohol consumption frequency (times per month, 0–30) and other health characteristics, including cardiovascular risk factors and mental distress. Relations were assessed using linear regression and reported as unstandardised beta coefficients [95% confidence interval (CI)].
Results The mean ± s.d. frequency of total alcohol consumption in the sample was 4.0 ± 3.8 times per month. In the low, medium, and high group of ability, the frequencies were 3.0 ± 3.3, 3.7 ± 3.5, and 4.7 ± 4.1, respectively. In the full sample, alcohol consumption was associated with physical activity, heart rate, fat mass, smoking, and mental distress. Most notably, each additional day of consumption was associated with a 0.54% (0.44–0.64) and 0.14% (0.09–0.18) increase in the probability of current smoking and mental distress, respectively. In each strata of ability (low, medium, high), estimates were 0.87% (0.57–1.17), 0.48% (0.31–0.66) and 0.49% (0.36–0.62) for current smoking, and 0.44% (0.28–0.60), 0.10% (0.02–0.18), and 0.09% (0.03–0.15) for mental distress, respectively.
Conclusions Participants with low cognitive ability drink less frequently, but in this group, more frequent alcohol consumption is more strongly associated with adverse health characteristics.
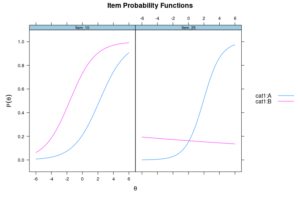
They unfortunately did the modeling backwards for intelligence:
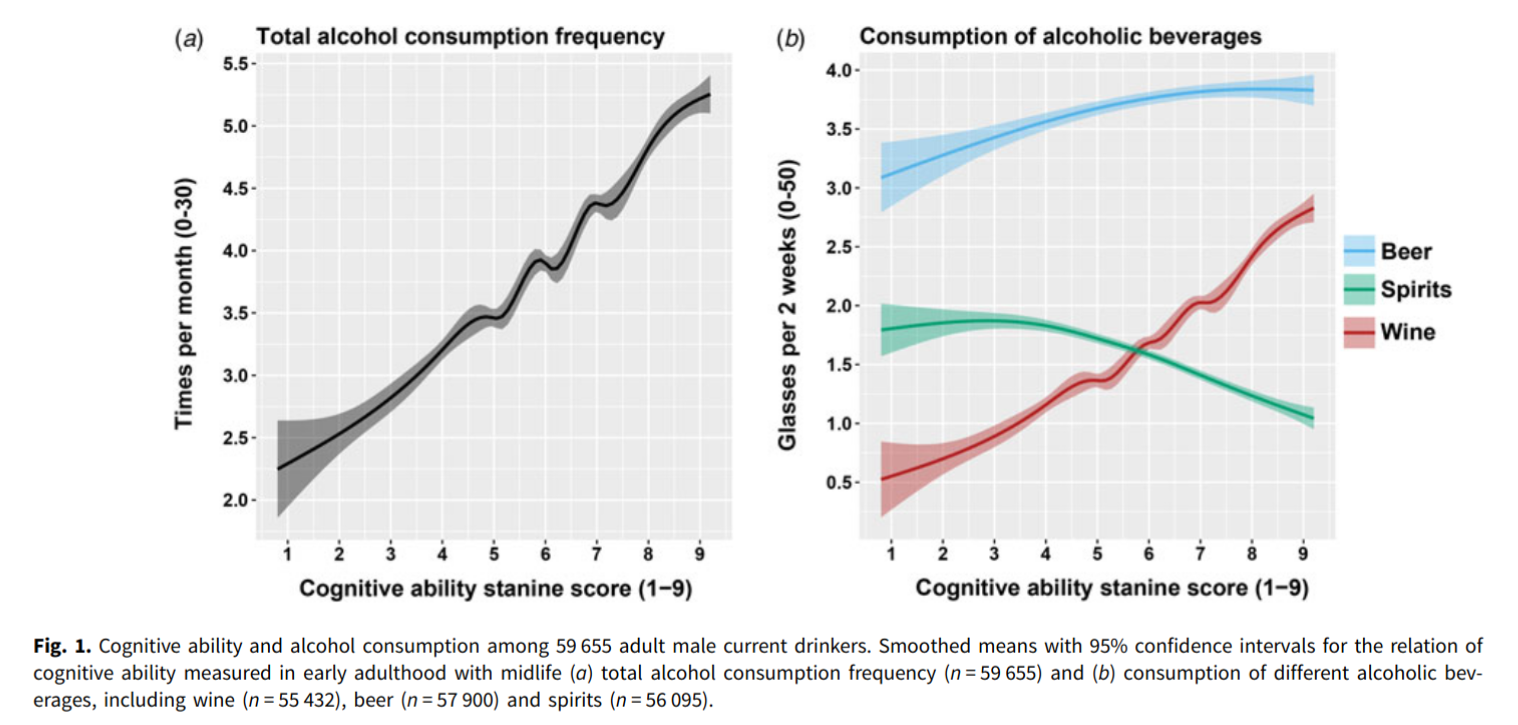
So here we see again that higher intelligence predicts more alcohol use, and changes the type too. Wine is indeed a mark of higher intelligence compared to spirits (hard liquor).

For the other variables, they put alcohol consumption as a the predictor. Here we see that more consumption relates to more problems at high levels, but if you look closely you see that some functions are slightly negative to begin with so that people who drink some alcohol are better off than people who don’t drink at all, and worst off are the people who drink a lot. This is most important for the mental distress outcome, but can also be seen for heart rate and physical activity. The latter two sound to me like an indicator of extroversion. Interesting, alcohol use has a mostly negative relationship with BMI, even at high levels. Alcoholics apparently don’t get so fat, maybe because they mostly substitute food for alcohol and end up not eating enough. To be fair, some variables don’t show any reversals, such as divorce, though it has a plateau for alcohol consumption around 7 glasses per month.
And because everything gets better with genetics, there is this recent GWAS:
- Johnson, E. C., Demontis, D., Thorgeirsson, T. E., Walters, R. K., Polimanti, R., Hatoum, A. S., … & Wang, J. C. (2020). A large-scale genome-wide association study meta-analysis of cannabis use disorder. The Lancet Psychiatry, 7(12), 1032-1045.
Background Variation in liability to cannabis use disorder has a strong genetic component (estimated twin and family heritability about 50–70%) and is associated with negative outcomes, including increased risk of psychopathology. The aim of the study was to conduct a large genome-wide association study (GWAS) to identify novel genetic variants associated with cannabis use disorder.
Methods To conduct this GWAS meta-analysis of cannabis use disorder and identify associations with genetic loci, we used samples from the Psychiatric Genomics Consortium Substance Use Disorders working group, iPSYCH, and deCODE (20 916 case samples, 363 116 control samples in total), contrasting cannabis use disorder cases with controls. To examine the genetic overlap between cannabis use disorder and 22 traits of interest (chosen because of previously published phenotypic correlations [eg, psychiatric disorders] or hypothesised associations [eg, chronotype] with cannabis use disorder), we used linkage disequilibrium score regression to calculate genetic correlations.
Findings We identified two genome-wide significant loci: a novel chromosome 7 locus (FOXP2, lead single-nucleotide polymorphism [SNP] rs7783012; odds ratio [OR] 1·11, 95% CI 1·07–1·15, p=1·84 × 10−9) and the previously identified chromosome 8 locus (near CHRNA2 and EPHX2, lead SNP rs4732724; OR 0·89, 95% CI 0·86–0·93, p=6·46 × 10−9). Cannabis use disorder and cannabis use were genetically correlated (rg 0·50, p=1·50 × 10−21), but they showed significantly different genetic correlations with 12 of the 22 traits we tested, suggesting at least partially different genetic underpinnings of cannabis use and cannabis use disorder. Cannabis use disorder was positively genetically correlated with other psychopathology, including ADHD, major depression, and schizophrenia.
Interpretation These findings support the theory that cannabis use disorder has shared genetic liability with other psychopathology, and there is a distinction between genetic liability to cannabis use and cannabis use disorder.
The key figure is:

The key here is to look for the lines where the circles, which represent cannabis use, are different from the diamonds which are cannabis abuse/addiction. So for BMI, using cannabis relates to lower BMI, but having a disorder relates to higher BMI. This is also the case for educational attainment, which recall, is mostly a proxy for intelligence and some personality traits. Comparing the various psychiatric diagnoses also shows the circles are to the left of the diamonds, so they are less strongly related to mental issues. The only exception here is for anorexia, but that doesn’t surprise us because anorexia is positively associated with intelligence: anorexics are actually 8 IQ higher on average, which is a lot!
They even used polygenic scores and related this to white brain matter in children in the ABCD:

We can clearly see the divergence between problem users and regular users.
Finally, for good measure, here’s the OKCupid database (public!) results which I computed just for this post. There’s more than one question about drug use of various sorts, but they tell a consistent story. Here’s alcohol:

The sometimes drinkers are higher intelligence than the never drinkers.
Drugs in general:

Often users are probably lower than sometimes users.
Psychedelics:

Never users are lower intelligence than users, but psychedelic-curious are the highest. The top category is probably some combination of druggies and regular users. This finding is somewhat inconsistent with that of the first study. My hypothesis for this is that OKCupid users are young, so they haven’t had enough time yet to try psychedelics and for the full pattern to emerge.
And then the usual “hard drugs”:

Regular users are much lower, but otherwise users are higher intelligence than nonusers.
Conclusions
- Drug use does not look universally, monotonically bad judging from the various correlates. Rather, too much drug use is a problem, but drug curiosity is probably a good thing.
- Various datasets and methods confirm the same kind of pattern.
- Questions can be raised about drug policies that blankly ban drugs for everyone even though most people don’t get into problems. It would seem that our law is intended to stigmatize it overall so that a minority of problem users can be legally targeted to prevent their self-harm, and everybody else has to suffer a fine once in a while. I don’t think this is the optimal policy.