This one keeps coming up whenever I post things about mental illness and X, like politics. So it’s worth having a go-to summary for a popular audience.
Mental illness is generally classified as membership of a bunch of discrete categories with either/or status. This is true whether one uses the DSM system or the ICD one. We also know that mental illness does not really conform to such a taxonomic system. There is a research field dealing with this stuff called nosology, which you can easily find on Google Scholar. The two most promising replacements for this old categorical system are the latent variable approach and the network psychometrics approach (which is very cool). The second approach is less used and I don’t know of any studies relating it to intelligence, but we already know results are almost equivalent at the score level, so the results cannot differ much, and thus are not of interest to us here.
The latent variable approach follows the approach well known from personality psychology, intelligence research, and pretty much all other modern psychology. One notes that mental illness measures, whether categorical or symptom scale (semi-continuous based on a score list like this one), are actually correlated, so that anyone with one diagnosis is at elevated risk of pretty much every other diagnosis. Still, some diagnosis go more commonly together (say anxiety and depression), which means one can also cluster them. The typical model is that of the general factor of psychopathology (Greek for mental illness), called the P factor, and which has various sub-factors for diagnosis that are more related than expected based on the general factor. Here I draw from one particularly nice 2014 paper but this 2020 review is also nice:
- Caspi, A., Houts, R. M., Belsky, D. W., Goldman-Mellor, S. J., Harrington, H., Israel, S., … & Moffitt, T. E. (2014). The p factor: one general psychopathology factor in the structure of psychiatric disorders?. Clinical psychological science, 2(2), 119-137.
Mental disorders traditionally have been viewed as distinct, episodic, and categorical conditions. This view has been challenged by evidence that many disorders are sequentially comorbid, recurrent/chronic, and exist on a continuum. Using the Dunedin Multidisciplinary Health and Development Study, we examined the structure of psychopathology, taking into account dimensionality, persistence, co-occurrence, and sequential comorbidity of mental disorders across 20 years, from adolescence to midlife. Psychiatric disorders were initially explained by three higher-order factors (Internalizing, Externalizing, and Thought Disorder) but explained even better with one General Psychopathology dimension. We have called this dimension the p factor because it conceptually parallels a familiar dimension in psychological science: the g factor of general intelligence. Higher p scores are associated with more life impairment, greater familiality, worse developmental histories, and more compromised early-life brain function. The p factor explains why it is challenging to find causes, consequences, biomarkers, and treatments with specificity to individual mental disorders. Transdiagnostic approaches may improve research.
Their main models:

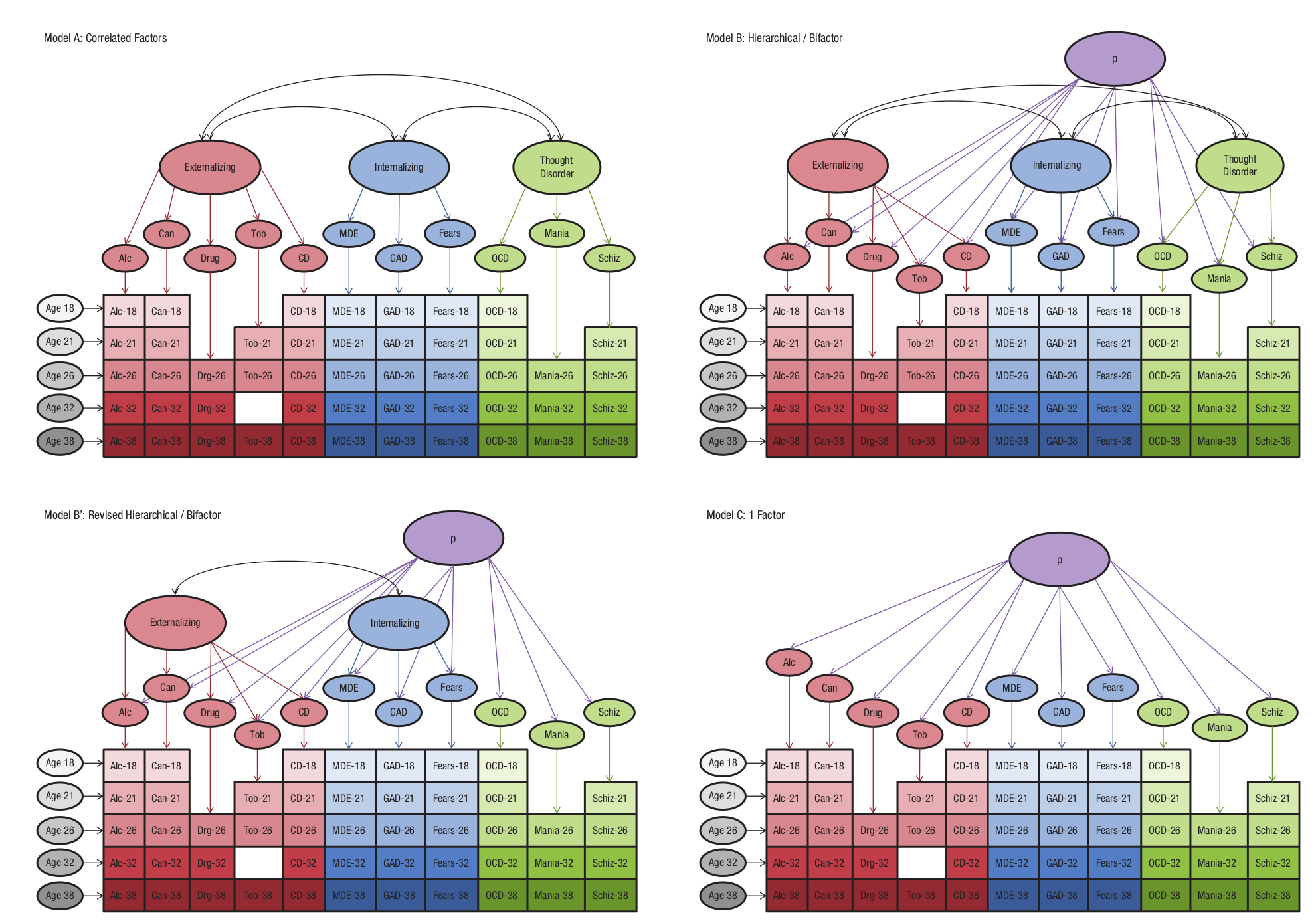
OK, so there are four models, authors explain:
The structure of psychopathology Three models were tested using confirmatory factor analysis: a correlated-factors model (Model A), a hierarchical or bifactor model (Model B), and a 1-factor model (Model C) Model B′ shows the final revised hierarchical model Colored ovals represent latent (unobserved) continuous symptom trait factors colored boxes represent observed symptom counts for each disorder at each assessment age The following 11 disorder/symptoms were assessed alcohol dependence, cannabis dependence, dependence on hard drugs, tobacco dependence, conduct disorder, major depression, generalized anxiety disorder, fears/phobias, obsessive-compulsive disorder, mania and positive and negative schizophrenia symptoms. Disorder/symptoms were assessed at ages 18, 21, 26, 32, and 38 years (not all disorders were assessed at every age, but each disorder was measured at least three times; missing assessments are depicted by white space) Gray ovals represent method/state factors designed to pull out age- and assessment-related variance (e.g., interviewer effects, mood effects, and age-specific vulnerabilities) that was uncorrected with trait propensity toward psychopathology. Note Alc = alcohol; Can = cannabis; Drg = hard drugs Tob = tobacco; CD = conduct disorder; MDE = major depression; GAD = generalized anxiety disorder; Fears = fears/phobias; OCD = obsessive-compulsive disorder; Schiz = schizophrenia
So the TL;DR is that they measured symptoms (the numerical score) for each of these disorders at different ages. When analyzed, they form 3 main clusters (externalizing, internalizing, and thought disorder), and the clusters are still correlated, so there is a higher order factor one can posit, the general P factor. One can use some model fit statistics to attempt to pick between these models, but generally speaking, it is best to use the bi-factor model since this leads to easily interpretable scores (the factor scores are orthogonal). The hierarchical model can also be turned orthogonal using the Schmid Leiman transformation, which then makes them essentially identical to the bi-factor.
Anyway, so once one has this data, one can compute the correlations of scores on P (general factor), Ext (externalizing), Int (internalizing), TD (thought disorder) to intelligence scores or anything else really. A correlation with P is what it means to say that something relates to mental illness in general. In many datasets, one will not have a nice P factor based on many diagnosis or diverse items, so one can use some aspect of P, such as depression, as as proxy. This will introduce some less of signal and maybe bias if this particular diagnosis has an additional relationship to the variable of interest beyond its association with P.
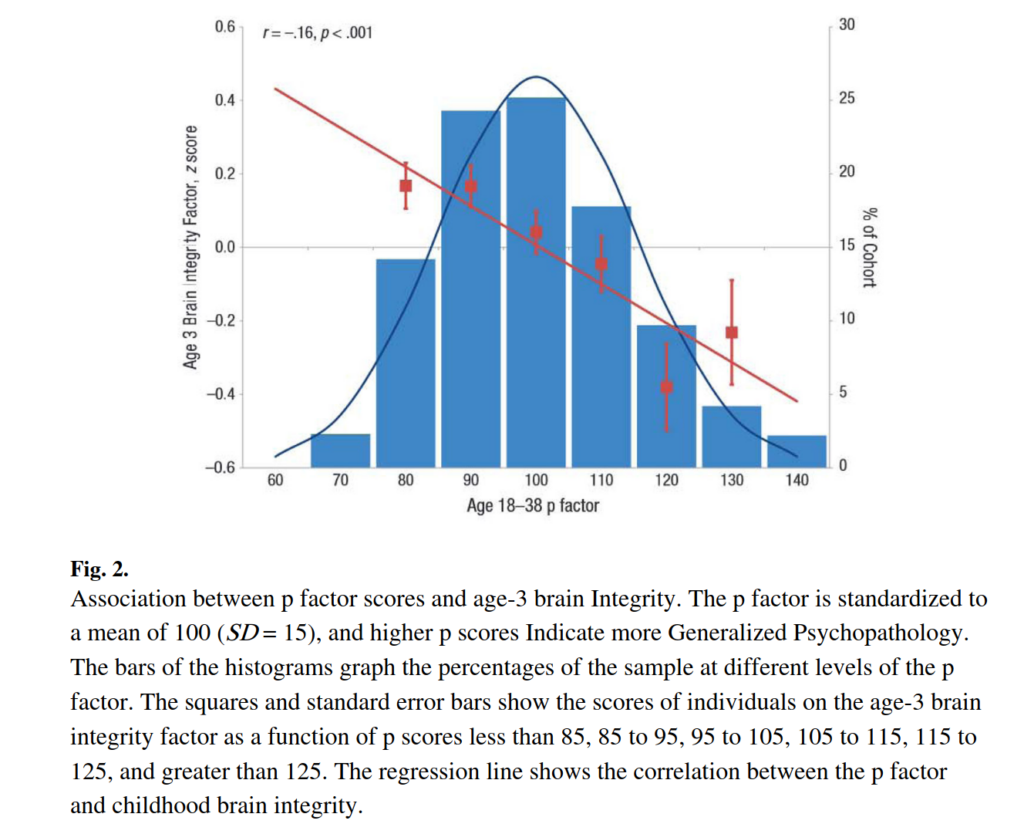
Returning to the main topic at hand, luckily, this same 2014 study reports a bunch of correlations we can draw on. The authors cryptically has an brain integrity factor, which sounds like absence of brain trauma or something, but it is actually just intelligence under another name (we know this game by now):
Their results are detailed in Table 2, which is very very long so I had to merge it:

OK, so they have some large number of intelligence measures at different ages. We really only care about the best overall estimates, which are: the WAIS-4 (i.e. adult scores), which show r = -.19, the age 7-11 WISC shows -.15, and the age 3 composite shows -.16. So everything is consistent and fairly similar in size, with some suggestion that the adult is stronger. For good measure, they also show social class is at -.14, somewhat weaker than the intelligence measures.
This is a decent sized study (New Zealand’s Dunedin sample, n = 1000ish), but we still want replication, so I looked and here’s the best one can get — a Nordic register study:
- Pettersson, E., Lichtenstein, P., Larsson, H., D’Onofrio, B. M., Lahey, B. B., & Latvala, A. (2021). Associations of resting heart rate and intelligence with general and specific psychopathology: a prospective population study of 899,398 Swedish men. Clinical psychological science, 9(3), 524-532.
We examined longitudinal associations of resting heart rate (RHR) and general intelligence (IQ) with two psychopathology models (correlated factors and general factor model). RHR and IQ were measured during conscription (mean age = 18.23 years; N = 899,398 Swedish males). A correlated factors model of register-based outcomes (including 10 psychiatric diagnoses, criminal convictions, and prescription of anxiolytic medications; mean age at follow-up = 43.09 years) identified internalizing, externalizing, and psychotic dimensions; the general factor model additionally identified a general dimension. All correlated factors were inversely associated with IQ; however, the general factor model showed that several of these associations were attributable to general variance rather than specific variance. In both psychopathology models, RHR weakly but significantly predicted higher internalizing but lower externalizing problems. Intelligence might be a transdiagnostic risk factor for any form of psychopathology, and the internalizing and externalizing spectra might be differentiated by psychobiological processes related to sensitivity to punishment.
Their factor loadings:
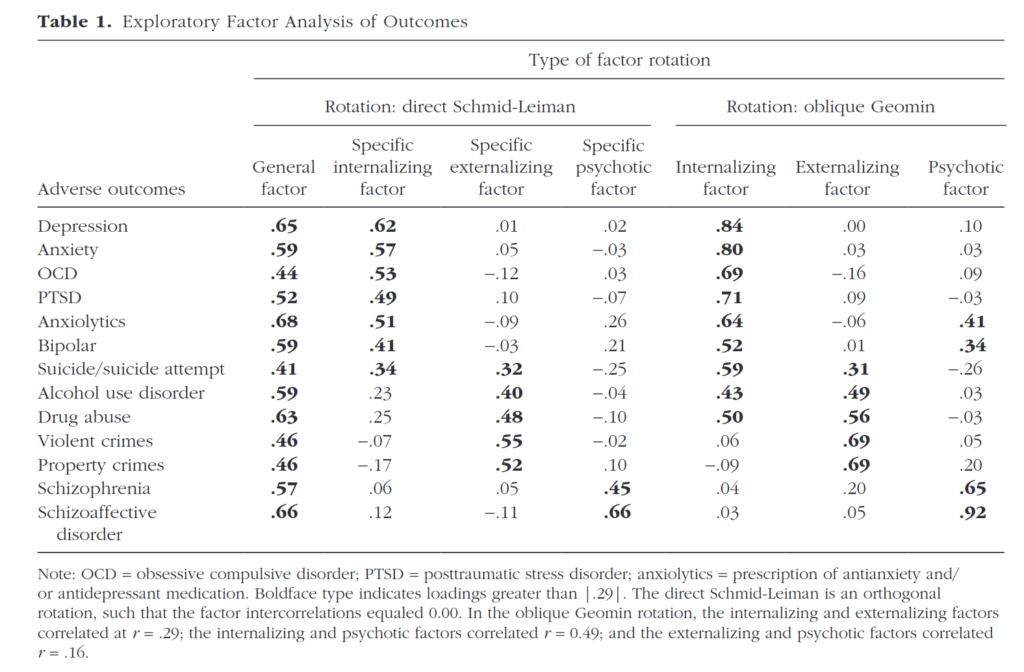
Schmid-Leiman is basically the same as bi-factor model, so the general factor in the left column is what we care about. How does it relate to intelligence? Authors opted for a regression model with some other stuff:
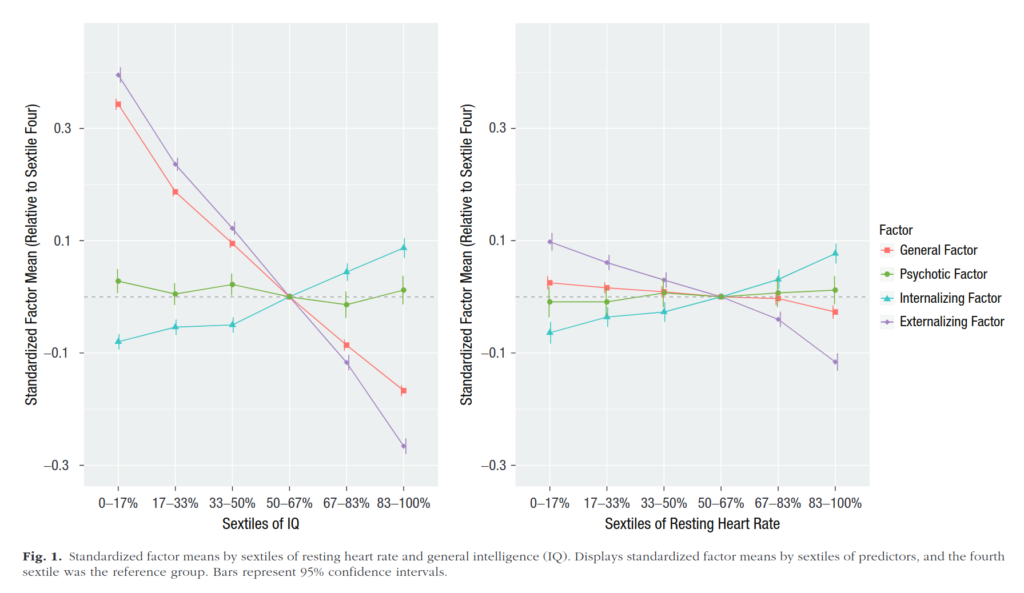
Hard to read? Yeah a little bit. The left plot has IQ sextiles (6-way split), so the top 83-100 centiles (IQ’s >114) have a P factor score at some 0.6 SD lower than the lowest group (IQ’s <86). The externalizing factor also shows a strong pattern by itself, while the other factors don’t (that is, one you remove the P factor variance from them). In numbers:
First, we regressed the general factor model onto RHR, IQ, and the covariates (RMSEA =0.008, 90% CI = [0.007, 0.008]; CFI = .994; TLI = .993; χ2(148) = 13,063.714, p < .001). The results are displayed in Table 1. RHR had a small but significant effect on the general factor (β= −0.010, 95% CI = [−0.014, −0.006]). Furthermore, RHR significantly predicted higher specific internalizing problems (β = 0.040, 95% CI = [0.034, 0.046]) and higher specific psychotic problems (β= 0.025, 95% CI = [0.017, 0.033]) but lower specific externalizing problems (β = −0.074, 95% CI = [−0.078, −0.070]). In contrast, IQ was a significant and negative predictor of the general factor of psychopathology (β = −0.181, 95% CI = [−0.183, −0.179]). Furthermore, IQ was negatively associated with the specific externalizing factors (β = −0.221, 95% CI = [−0.225, −0.217]) and specific psychotic factors (β = −0.015, 95% CI = [−0.021, −0.009]) and positively associated with the specific internalizing factor (β = 0.054, 95% CI = [0.050, 0.058]). The associations with the four latent factors (Fig. 1) and the 13 adverse outcomes (see Table S3 in the Supplemental Material) appeared largely linear.
The main value here to note is β = −0.181. The Dunedin study’s value was r = -.19 for the adult data, so the replication is extremely tight. We furthermore see that the pattern is very linearly (red line).
Even our favorite socialist intelligence researcher Kathryn Paige Harden has a replication:
- Harden, K. P., Engelhardt, L. E., Mann, F. D., Patterson, M. W., Grotzinger, A. D., Savicki, S. L., … & Tucker-Drob, E. M. (2020). Genetic associations between executive functions and a general factor of psychopathology. Journal of the American Academy of Child & Adolescent Psychiatry, 59(6), 749-758.
Objective:
Symptoms of psychopathology covary across diagnostic boundaries, and a family history of elevated symptoms for a single psychiatric disorder places an individual at heightened risk for a broad range of other psychiatric disorders. Both twin-based and genome-wide molecular methods indicate a strong genetic basis for the familial aggregation of psychiatric disease. This has led researchers to prioritize the search for highly heritable childhood risk factors for transdiagnostic psychopathology. Cognitive abilities that involve the selective control and regulation of attention, known as executive functions (EFs), are a promising set of risk factors.Method:
In a population-based sample of child and adolescent twins (n = 1,913, M age = 13.1 years), we examined genetic overlap between both EFs and general intelligence (g) and a transdiagnostic dimension of vulnerability to psychopathology comprising symptoms of anxiety, depression, neuroticism, aggression, conduct disorder, oppositional defiant disorder, hyperactivity and inattention. Psychopathology symptoms were rated by both children and their parents.Results:
Latent factors representing general EF and g were highly heritable (h2 = 86–92%), and genetic influences on both sets of cognitive abilities were robustly correlated with transdiagnostic genetic influences on psychopathology symptoms (genetic rs ranged from −.20 to −.38).Conclusion:
Both EF and g robustly index genetic risk for transdiagnostic symptoms of psychopathology in childhood. Delineating the developmental and neurobiological mechanisms underlying observed associations between cognitive abilities and psychopathology remains a priority for ongoing research.
So about 1900 twins of young age, and they find intelligence was ~90% heritable (!), and intelligence was correlated genetically with mental illness diagnoses and in general.
Finally, I just want to plug our own study of 4450 US veterans (VES). We found that intelligence correlates at -.35 with the general factor of the MMPI2, which is a good measure of P based on self-report. This value is about twice as high as the one others find, I don’t have any particular theory about why that is the case. Our sample was middle aged men who served in the US army.
Claims of higher mental illness in the very intelligent
This claim is common but largely false. Not entirely false, but largely. If we look at data from the ultra smart people, we do find elevated rates of loneliness and the like. Most famously, people will cite data from Termin’s study as written up by Grady M. Towers in his essay called The Outsiders. Looks like this:

The CMT-T is the concept mastery test, a very high range test, these are not normal IQs. Their measurement is defined as:
1. Satisfactory. Subjects classified in this category were essentially normal; i.e., their “desires, emotions, and interests were compatible with the social standards and pressures” of their group. Everyone, of course, has adjustment problems of one kind or another. Satisfactory adjustment as here defined does not mean perfect contentment and complete absence of problems, but rather the ability to cope adequately with difficulties in the personal make-up or in the subject’s environment. Worry and anxiety when warranted by the circumstances, or a tendency to be somewhat high strung or nervous–provided such a tendency did not constitute a definite personality problem–were allowed in this category. 2. Some maladjustment. Classified here were subjects with excessive feelings of inadequacy or inferiority, nervous fatigue, mild anxiety neurosis, and the like. The emotional conflicts, nervous tendencies and social maladjustments of these individuals, while they presented definite problems, were not beyond the ability of the individual to handle, and there was no marked interference with social or personal life or with achievement. Subjects whose behavior was noticeably odd or freakish, but without evidence of serious neurotic tendencies, were also classified in this category. 3. Serious maladjustment. a.) Classified as 3a were subjects who had shown marked symptoms of anxiety, mental depression, personality maladjustment, or psychopathic personality. This classification also includes subjects who had suffered a “nervous breakdown,” provided the condition was not severe enough to constitute a psychosis. Subjects with a previous history of serious maladjustment or nervous breakdown (without psychosis) were included here even though their adjustment at the time of rating may have been entirely satisfactory. b.) Classified as 3b were those subjects who had at any time suffered a complete mental breakdown requiring hospitalization, whatever their condition at the time of rating. In the majority of cases the subjects were restored to reasonably good mental health after a brief period of hospital care [6, pp. 99-101].
OK, so seems very contradictory to the population data right? Yes, I imagine being ultra smart in 1950 or somewhen was a very lonely experience, and this may lead to issues. But these people are extremely rare, so their experiences don’t really affect the general pattern we saw above in modern data. I also speculate that modern data would not show this pattern so strongly due to greater ease of connecting with other smart people nowadays (e.g. rationalist community, and really, anywhere intellectual on the internet).
There is another recent study looking into this matter, but it’s pretty dumb:
- Karpinski, R. I., Kolb, A. M. K., Tetreault, N. A., & Borowski, T. B. (2018). High intelligence: A risk factor for psychological and physiological overexcitabilities. Intelligence, 66, 8-23.
High intelligence is touted as being predictive of positive outcomes including educational success and income level. However, little is known about the difficulties experienced among this population. Specifically, those with a high intellectual capacity (hyper brain) possess overexcitabilities in various domains that may predispose them to certain psychological disorders as well as physiological conditions involving elevated sensory, and altered immune and inflammatory responses (hyper body). The present study surveyed members of American Mensa, Ltd. (n = 3715) in order to explore psychoneuroimmunological (PNI) processes among those at or above the 98th percentile of intelligence. Participants were asked to self-report prevalence of both diagnosed and/or suspected mood and anxiety disorders, attention deficit hyperactivity disorder (ADHD), autism spectrum disorder (ASD), and physiological diseases that include environmental and food allergies, asthma, and autoimmune disease. High statistical significance and a remarkably high relative risk ratio of diagnoses for all examined conditions were confirmed among the Mensa group 2015 data when compared to the national average statistics. This implicates high IQ as being a potential risk factor for affective disorders, ADHD, ASD, and for increased incidence of disease related to immune dysregulation. Preliminary findings strongly support a hyper brain/hyper body association which may have substantial individual and societal implications and warrants further investigation to best identify and serve this at-risk population.
So this one has both the obvious sampling bias of sampling Mensa members, and relying solely on self-report for diagnoses. Is anyone surprised at these findings? Everybody knows Mensa is full of dorks and otherwise unproductive people. Mensa members are not representative of smart people.
The author was told this issue by multiple people, including me, at the ISIR 2015 conference where she presented these findings, but somehow, 3 years later, this appears in print. I mean, OK, the paper does have a caveat about this in the discussion section, but the abstract has basically nothing. Editor must have liked the paper or got really lucky with the reviewers, who can say?
But Emil, I know so many smart and crazy people! How can this be if there is no positive association?
Have you ever considered that maybe, just maybe, you are also crazy and smart, and due to social homophily, that’s why you ended up with so many smart and crazy friends?
But Emil, so many geniuses were clearly crazy, and they are very smart, so how can this be?
Geniuses are very smart, but they are also other things, and not representative of smart people in general. A lot of research has found that geniuses have elevated rates of mental illness as well as elevated rates of mental illness in their families.