To be precise, exclusive homosexuality is. But let’s backtrack a bit. Scott Alexander has a new piece out that begins with this disclaimer:
CONTENT NOTE: This essay contains sentences that would look bad taken out of context. In the past, I’ve said “PLEASE DON’T TAKE THIS OUT OF CONTEXT” before or after these, but in the New York Times’ 2021 article on me, they just quoted the individual sentence out of context without quoting the “PLEASE DON’T TAKE THIS OUT OF CONTEXT” statement following it. To avoid that, I will be replacing spaces with the letter “N”, standing for “NOT TO BE TAKEN OUT OF CONTEXT”. If I understand journalistic ethics correctly, they can’t edit the sentence to remove the Ns – and if they kept them, people would probably at least wonder what was up.
I guess that means roughly the same as his old category of posts “things I will regret writing”. Scott’s argument is like this:
That N means N that N a N purely N biological N apolitical N taxonomy N of N mental N disorders N which N classifies N all N things N with N similar N biological N causes N in N the N same N way N would N also N probably N classify N homosexuality N as N a N mental N disorder. But the whole point of wanting a purely biological apolitical taxonomy of mental illness was to make sure we would never again repeat the DSM’s error of calling homosexuality a mental disorder!
So in brief: 1) DSM-3 and earlier used to classify homosexuality as a mental disorder, but DSM-4 removed this “in response to mounting pressure” (i.e. leftist activism). 2) But actually pedophilia and homosexuality are pretty similar biologically speaking, so both should be classified as mental illness or neither. Scott doesn’t want to bite the bullet and say that DSM unclassifying homosexuality was a mistake, so he has to go on complicating things about how classifications are also political, as they unlock monetary support for treatment. In the case of transgender people, that’s very important to them as their treatment is very expensive, and they want others to pay for it (hence using legal tricks like joining the army to have them pay for it). But then again, this is really just allowing politics to affect our scientific classification system. So Scott is really just saying that we shouldn’t consider DSM a purely scientific classification system, but rather a partially political one where some people get to have special status to suit their political goals.
I submit this is not a very, well, scientific approach. The correct solution is to recognize that homosexuality is a mental illness for the obvious reasons. As Scott mentions, it belongs to the sexual targeting group of problems. From an evolutionary perspective, humans are a sexually reproducing species, so sexuality should — must — be targeted at the opposite sex. But furthermore, it should be targeting the right age too. So since female fertility is strongly age-dependent, men’s targeting must be primarily of fecund females, so age 15-45 or so. Female targeting can be less age dependent, but should at least be 15+ (and that’s what we see). Thus, if someone is targeting persons outside of the adaptive age, that is a disorder of sorts. In practical terms, when this happens to be children, it causes problems and we have a term for it, pedophilia. But it could also be targeting too old people, so we call it gerontophilia. No one seems to care much about this. It’s not even classified in the DSM, probably because no one cares enough to lobby for its inclusion. Why bother if a few weirdos look at grannies on Pornhub?
Aside from the evolutionary angle, we also know that homosexuality fits well within the nomological network of mental illness. The most important fact about mental illness is that all the various diagnoses tend to occur together, called comorbidity. This is why one can speak of mental illness overall as a kind of trait, which we call general psychopathology, or P factor. Homosexuality relates positively to most mental problems, and for genetic reasons too. This shows up whenever people do family studies or GWASs of homosexuality. For instance, in the Ganna et al 2019 GWAS, we can find these genetic correlations:
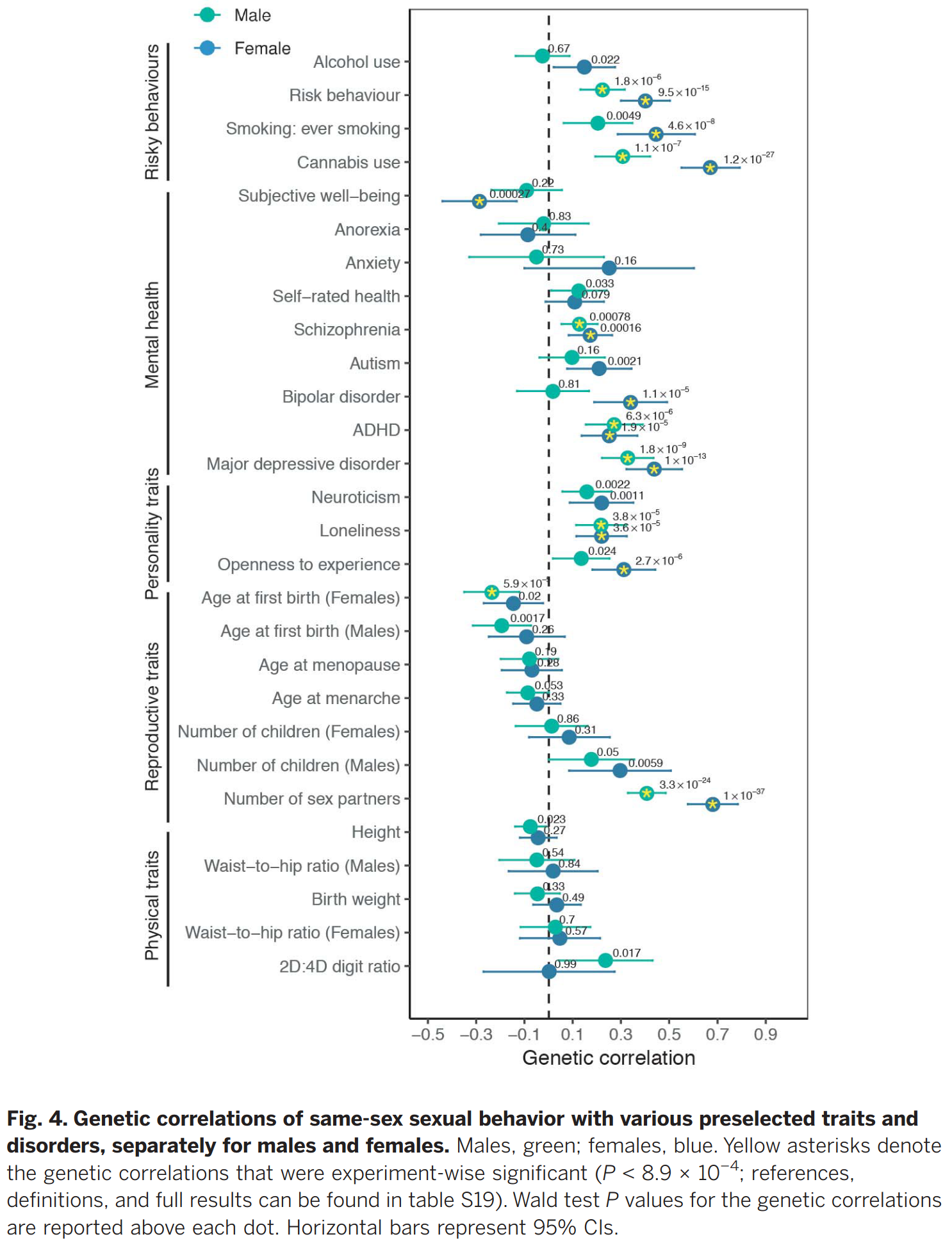
So homosexuality, not measured particularly well, shows genetic correlations with: schizophrenia, autism, bipolar, ADHD, depression, neuroticism, loneliness, but not with anxiety and anorexia. Two caveats here, aside from the questionable measurement in the dataset. First, just because a correlation is heritable (genetic), it doesn’t mean it has a straightforward intrinsic genetic explanation. So homosexuality could be related genetically to mental illness because other people treat homosexuals poorly, and that’s why they have bad mental health. This doesn’t really work though, and East Hunter goes through the evidence on his Substack. His conclusion:
I don’t think I became an instant expert on the minority stress hypothesis overnight. However, Ilan Meyer definitely is one, and these are the studies he cited in a recent (2020) paper in support, so my understanding is that this is the best evidence for it. If this is the case, then the minority stress hypothesis is on very weak footing. Most of this evidence is correlational and easily explained with things other than minority stress, for example selective migration of sexual minority members with better mental health. The pseudo-experimental results are underpowered, p-hacked and frankly often just deliberately misleading. It is clear that there is a very low standard for publishing “fancy design shows that progressive politics makes gay lives better” findings – authors, editors and funders all want these, while I assume it is much harder to publish negative findings in this topic.
So it’s pretty yawn tier evidence. But the more obvious unmentioned fact here is that stigma against homosexuals has decreased markedly in the last couple of decades, and yet homosexuals still show markedly elevated rates of mental problems. If this was caused by stigma, it should have declined rapidly, ergo, it is not caused by stigma. Sean Last also looked at discrimination and suicides and finds it not so convincing.
I don’t think this conclusion — that homosexuality is a mental illness — is as repugnant as it may seem. We classify depression as a mental illness, but no one goes around saying to stay away from depressed people, or not to love them. I submit the same is the case for homosexuality. Homosexuality is a net negative for a person, but humans can have so many problems. This is hardly the worst thing a friend or family member can have. Being schizophrenic, heavily autistic, or a drug abuser is probably a bigger problem.
So to return to Scott. His post is titled You Don’t Want A Purely Biological, Apolitical Taxonomy Of Mental Disorders, which thus is kind of correct. A correct biological classification would say that homosexuality, pedophilia, gerontophilia, “object sexuality” etc. are mental disorders of the class ‘targeting errors’, and since this is undesired by his readers, Scott is correct in saying that they don’t actually want that!
Does treatment for homosexuality work?
Of course, when we classify something as mental disorder, we say that it is better generally not to have it. As can be seen with all the associations with bad outcomes, this is generally true for homosexuality. There is of course also the added problems of being very low fertility (no grandchildren for mom!) and having more trouble finding suitable partners due to being limited to a small fraction of the dating pool. But we can treat psychosis, depression, anxiety and so on with some efficacy, so why not homosexuality? Well, it turns out there is a a published meta-analysis of papers that studied treatment back when this was allowed:
- Byrd, A. D., & Nicolosi, J. (2002). A meta-analytic review of treatment of homosexuality. Psychological reports, 1139-1152.
is paper examined and synthesized studies of treatment of individuals identified as homosexual using mera-analytic technique. A large number of studies (146) evaluating treatment efficacy were identified, most published prior to 1975 and 14 of which met inclusion criteria and provided statistics that could be used in a meta-analysis. These 14 outcome studies were published between 1969 and 1982 and used behavioral interventions. Analysis indicated that treatment €or homo- sexuality was significantly more effective than alternative treatments or control groups for homosexuality (ES = .72), and significant differences were found across pre- to postanalysis (ES=.89). In other words, the average patient receiving treatment was better off than 79% of those in the alternative treatments or as compared to pretreatment scores on the several outcome measures. This meta-analysis of 14 studies provides empirical support for a group of 146 studies which have narratively suggested that treatment for homosexuality is effective. Variables related to treatment efficacy are examined.
I am kinda surprised it has not received much attention, having only 49 citations since 2002 despite being a provocative piece. And still not retracted either! Whatever the reason, here’s the studies they included:

Neither the meta-analysis of the literature is convincing by modern post-replication crisis standards — but not much is!

So 14 studies with a mean sample size of 25, and they used something like 14 different designs and maybe half that different measures. Ripe for publication bias and p-hacking. Still, they managed to obtain an absurdly (?) large mean effect size of 0.89 d. And some of the studies used outcomes that are not so obviously stupid such as penile volume measures. I mean, I was expecting them to just rely on self-reported sexual behavior or thoughts following extended talks with priest-therapists. It would be easy to see how social desirability bias could distort such results. So maybe, just maybe, it isn’t as obviously stupid as it sounds. After all, if homosexuality can rapidly increase in the population, this suggests it can be environmentally induced, and in that case, maybe also cured (see also this post by George Francis). Oh and if you don’t like the 2002 meta-analysis, there’s a 2021 review written from a pro-LGBT angle which found 35 studies, but didn’t quantitatively synthesize them.

One question is whether one can treat it, the other question is whether the patients want it? And maybe there are some surveys of homosexuals that asked them if they would prefer to be heterosexual if they could. I didn’t see any published in the academic literature but here’s some anecdotes.

And of course, one can find endless numbers of papers with titles like What’s Good about Being Gay?.
Genetics and homosexuality and evolution
What about the heritability? Massive changes in recent historical time suggests a low heritability, but we also know that height can be some 95% heritable and still show a big change over the last 150 years. Here’s a good twin study on homosexuality (and here’s another):
-
Långström, N., Rahman, Q., Carlström, E., & Lichtenstein, P. (2010). Genetic and environmental effects on same-sex sexual behavior: A population study of twins in Sweden. Archives of sexual behavior, 39, 75-80.
There is still uncertainty about the relative importance of genes and environments on human sexual orientation. One reason is that previous studies employed self-selected, opportunistic, or small population-based samples. We used data from a truly population-based 2005–2006 survey of all adult twins (20–47 years) in Sweden to conduct the largest twin study of same-sex sexual behavior attempted so far. We performed biometric modeling with data on any and total number of lifetime same-sex sexual partners, respectively. The analyses were conducted separately by sex. Twin resemblance was moderate for the 3,826 studied monozygotic and dizygotic same-sex twin pairs. Biometric modeling revealed that, in men, genetic effects explained .34–.39 of the variance, the shared environment .00, and the individual-specific environment .61–.66 of the variance. Corresponding estimates among women were .18–.19 for genetic factors, .16–.17 for shared environmental, and 64–.66 for unique environmental factors. Although wide confidence intervals suggest cautious interpretation, the results are consistent with moderate, primarily genetic, familial effects, and moderate to large effects of the nonshared environment (social and biological) on same-sex sexual behavior.
But of course, evolution should tend to select against it very strongly as the fertility of homosexuals is very low. I computed some values previously in the GSS (American data):

Eye-balling, looks like male fertility is reduced by 80% or so, and female only by 60%. And this is by self-report. Obviously, if you never have sex with opposite sex people, your fertility is 0 (aside from modern things like donating or receiving sperm which did not exist in natural times). So why do we have so many of homosexuals? It’s not just humans, after all. There are many observations of same-sex behavior in animals too. So, homosexuality at least to some degree can definitely be natural, but we can also induce it.
Aside from the gay germ theory, which I think is not likely, unless it’s a metaphor for ‘grooming’, the other popular theory is sexual antagonistic selection. The idea here is that some genetic variants cause men to be gay, but increase fertility in their female relatives enough to make up for this. Or make the gays so helpful to relatives that their own fertility reduction is worth it. This is not impossible, but it is unlikely given the massive fertility loss we see above. Fortunately, we don’t have to speculate. There is a 2012 study that supports this and with dodgy p-values. But this much larger Dutch register study finds that homosexuals have fewer siblings, so their mothers don’t to be benefit from any hypothetical extra-fecundity genes, in fact the opposite. And this study shows that gay men actually help their families less then heterosexuals. I mean, is it so surprising? Gays are usually heavily into hedonism, not family making.
Conclusions
- Homosexuality is really a mental illness, that was declassified as such for the usual political leftism reasons. It fits well with other mental problems, and these are not plausibly caused by social factors.
- There is some old dodgy evidence that treatment for homosexuality works, and this evidence should be scrutinized anew.
- I don’t know what the demand is for treatment, but we should find out. I’m sure many parents would prefer to have grandchildren, for obvious evolutionary reasons, so probably some people would want treatment.
- The heritability also allows one to select embryos to be less likely to be gay.
- The evidence for gay germ theory, helpful uncle theory, and sexual antagonistic selection is weak at best.
- I don’t think that classifying homosexuality as a mental illness should change the behavior of heterosexuals much. Everybody has some friend who suffers from mental problems, and this is worthy of our sympathy without having to pretend it isn’t really a disorder.