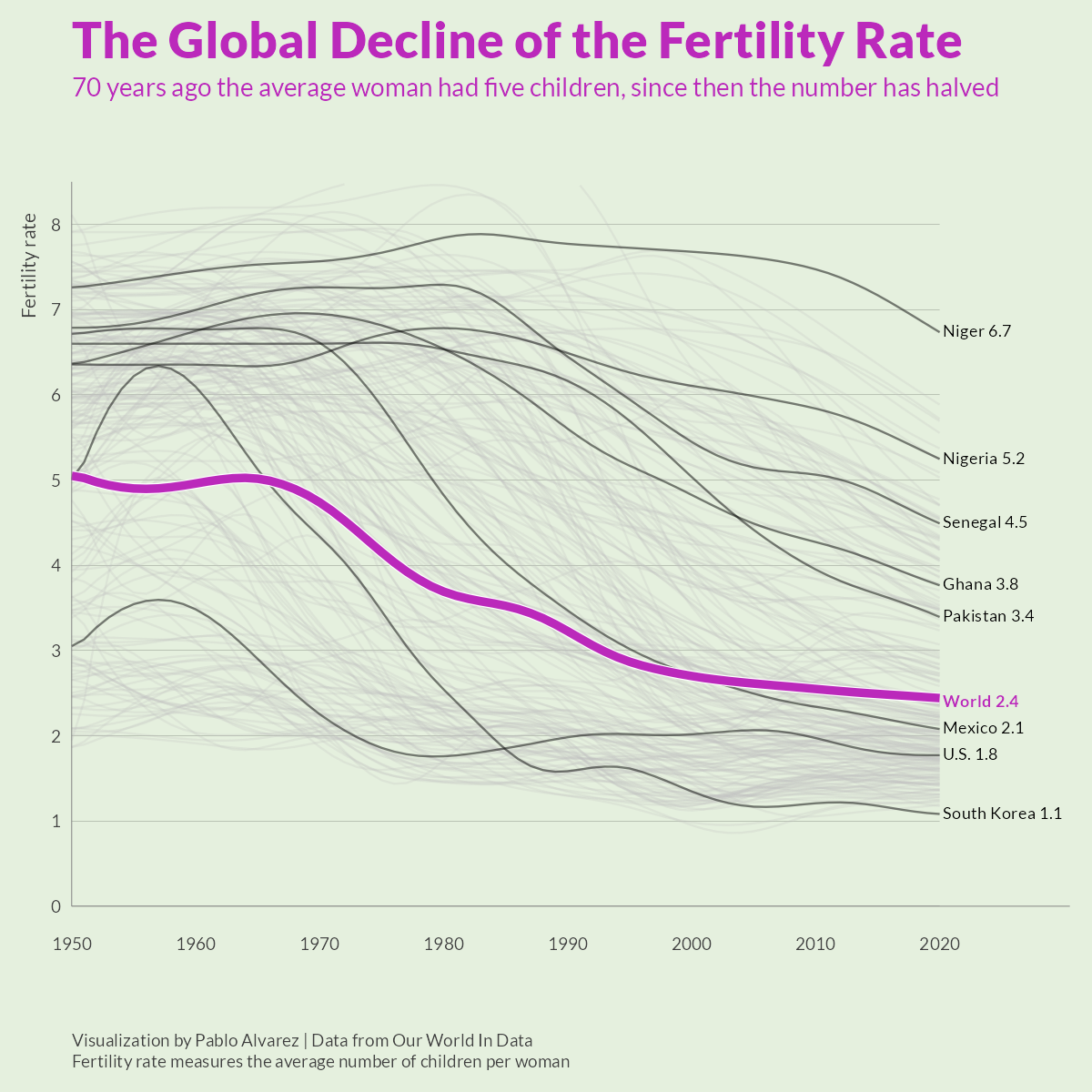
There is a worldwide decline in fertility:
The COVID-19 years seem to have been particularly bad on some countries. The poster child for future problems is South Korea:

Even Reuters is running scare stories for South Korea:
As a matter of fact, Best Korea’s fertility is also declining, prompting their dictator Kim Jong Un to cry on TV:
And the richest guy in the world — generally an optimist — is concerned about the fertility decline:

Alright, with the scene set, what do we know about fertility causes? Here’s an incomplete list in no particular order:
- Women’s labor market participation → lower fertility
- Long educational duration → lower fertility
- Non-religiousness/secularization → lower fertility
- Left-wing ideology → lower fertility
- Including climate worries and overpopulation worries in general
- Abortion availability → lower fertility
- Contraception availability → lower fertility
- Fertility role models → fertility changes
- Population density → lower fertility?
In this post I primarily want to attack the main cope theory of lower fertility — that people don’t have enough money — and push the last causal factor. But let’s ‘quickly’ go over the others.
Women’s labor market participation
People have a limited about of time to spend. Hence, time spent doing one thing can’t be spent doing something else (opportunity cost). Adults in the breeding age, say, 20-40, primarily spend their time on higher education and careers. Women’s role is here critical, as they must be the primary caregivers, so they are the ones who have to make a “sacrifice” in their careers in order to do this, whereas men can more easily delay it and don’t bear as much of the childcare burden and no pregnancy. As such, it is not surprising that women’s labor market participation, both in terms of being employed at all and number of hours worked per week, is a strong causal factor in their fertility. Empirically, looking at this is complicated because countries differ in their overall labor market participation rate for various reasons, as does their female participation rate, and the other causes of these rates can differ from the causes of fertility, making the pattern hard to see between countries. For a study on this, see Fertility and women’s employment reconsidered: a macro-level time series analysis for developed countries, 1960-2000. Overall, though, it is hard to deny the causality based on the reasoning, even if it can be hard to empirically prove with time series data using country level data.
Long education duration
Similar to above, time spent in higher education means fewer years on the job market before starting a family. Many women decide to delay family formation until their careers ‘get going’. In many cases this leads to a smaller number of children, as they hit their low fertility years before they start, and in some cases, no children at all despite desiring them. It’s possible to look at this using causally informative methods, such as policy reforms. One study from Greece (Higher education and fertility: Evidence from reforms in Greece):
This paper examines the impact of higher education on women’s fertility decisions. To address the endogeneity of non-compulsory education participation, I focus on an increase in the supply of higher education and a concurrent schooling reform that jointly expanded higher education opportunities in Greece in year 2000. Drawing data from the 10% sample of the 2011 Population Census, I use the exogenous variation introduced by the first grade enrollment age cutoff to apply a Regression Discontinuity Design comparing educational attainment and fertility for women that were just, and just not exposed to the reforms. The probability of giving birth before age 30 decreases by around 20 percentage points for women who completed higher education because they were exposed to the reforms. Career outcomes for employed women with higher education improve, while fertility decreases at ages following graduation, suggesting that the result is primarily driven by the increasing opportunity cost of children.
Visually, it doesn’t look that impressive, but the p-values were good (everything < .01):

Religiousness and fertility
I’ve written about this one before when explaining our Mormon eugenics or dysgenics resistance study. Religious people have quite a bit higher fertility in general. As the world religiousness declines, so does the fertility. The causality is plausible because most successful religions include explicitly pro-natalism teachings, e.g. in Genesis “Be fruitful and multiply; fill the earth and subdue it” (anti-natalist religions unsurprisingly die out). Many religions also include bans or limitations on contraception and abortion, famously the Catholic church (even if these are not followed 100%, they have some effect). There are tons of plots floating around the internet about this, here’s one for USA based on church attendance:

Eric Kaufmann wrote an entire book based on extrapolation this idea, Shall the religious inherit the earth? (answer: yes, but give it a hundred years or so):

We might also wonder whether the more backwards/less liberal/more fundamentalist religions have a stronger fertility effect. The answer seems to be… kinda sorta, used to be? Here’s a study comparing various religious groups in Europe over time (Religiousness and Fertility among European Muslims):

So Muslims have higher fertility, but their advantage is going away. It’s very clear when we look at Slovenian data over time:

Muslims used to have over twice the fertility of Catholics (2.5 more on average), but in the birth cohorts of 1962-1966, this was only 0.19 children more on average. Granted, in percentage terms, it’s still notable (+10%), but it’s not what it used to be (+115%). This pattern is general, second generation non-Western (mainly Muslim) immigrants tend to converge with national fertility levels. Here’s the Danish experience:

The orange line shows 1st generation non-Western immigrants, who were having more than 3 children per woman until around 2000, then started a decline, and now are having about 1.5 or so, the same as everybody else except for Western 1st generation immigrants, who are a bit lower. Islam, as such, might have been a potent source of pro-natalism, but not anymore. The same pattern can be seen if we look at Muslim countries:
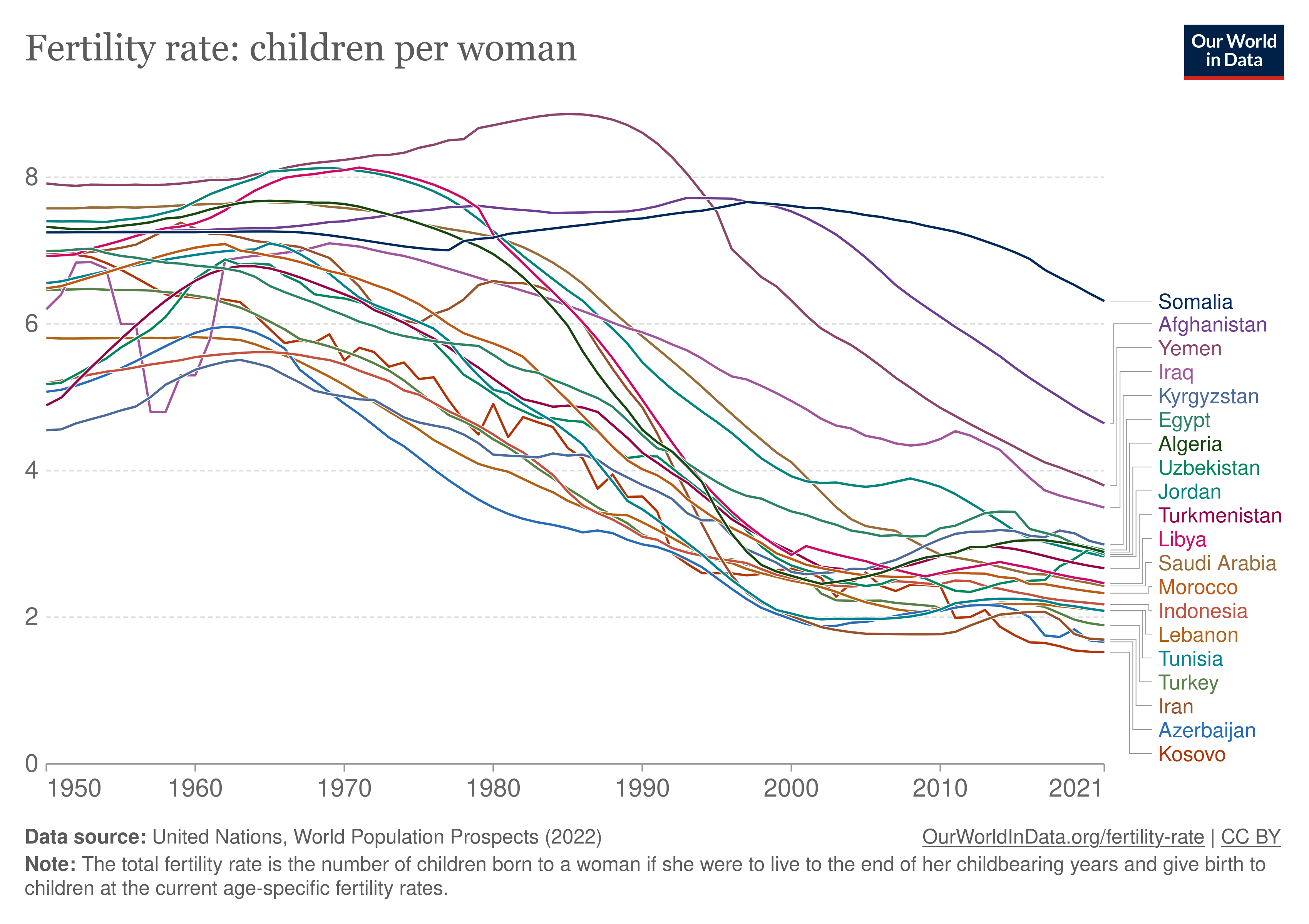
Even within Israel, the Muslims have stopped having an advantage in fertility:

Fears of Muslims outbreeding Christians in their own countries, then, can be put to rest. They appear to be affected by the same causes of lower fertility just about as much as everybody else where they live. Islamification of Western countries, then, comes down mainly to new immigration (plus the demographic momentum).
Left-wing ideology
I’ve also covered this one before, but briefly, in recent decades, conservatives have started to outbreed lefties (data from the USA, GSS, see Political Attitude and Fertility: Is There a Selection for the Political Extreme?):

Thus, it seems conservative advantage in fertility is only there since the 1990s, perhaps about the same religiousness got associated with political conservatism in the USA. The authors didn’t adjust for race or religiousness, so I don’t know if this mixed pattern has something to do with changing fertility rates by race in the USA.
Abortion availability
This one is more obvious, and as usual, we can find some dramatic looking plots floating around on Twitter. Here’s one from a study of Romania’s communists banning and re-legalizing abortion (The Impact of Legalized Abortion on Child Health Outcomes and Abandonment. Evidence from Romania):
![]()
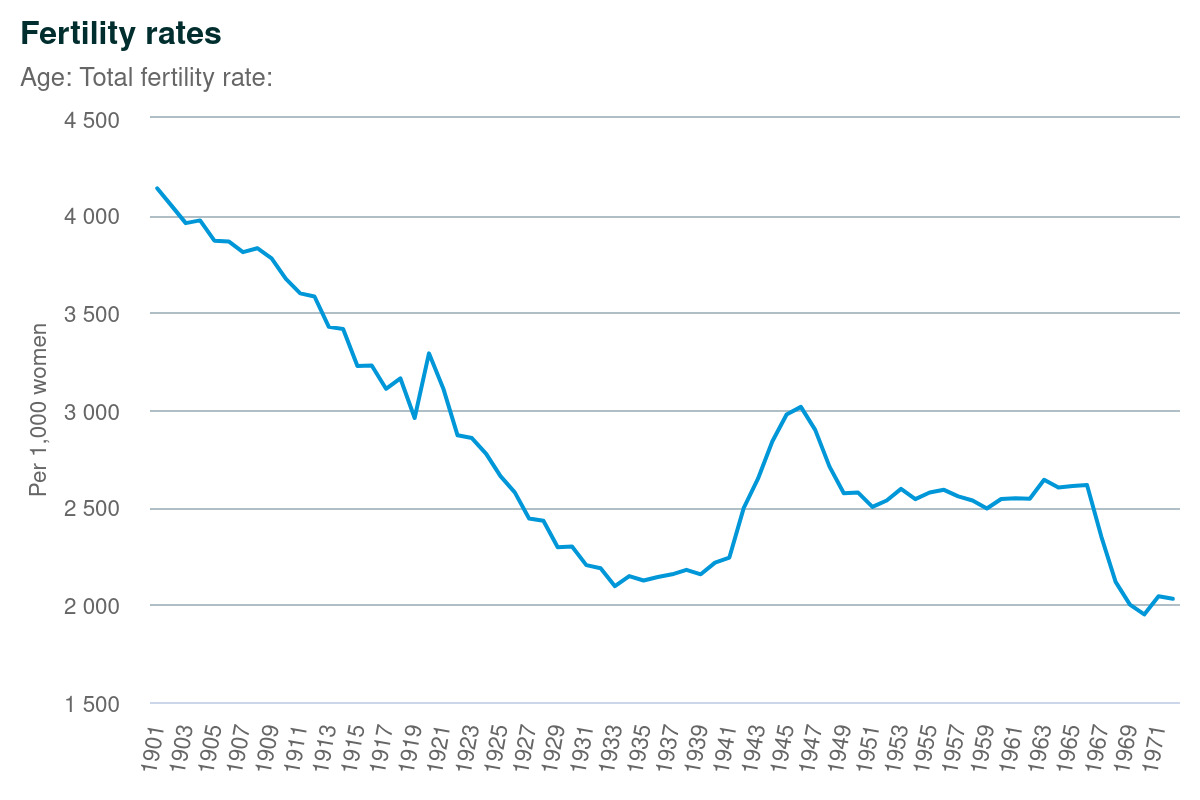
One could add other examples (UK data):
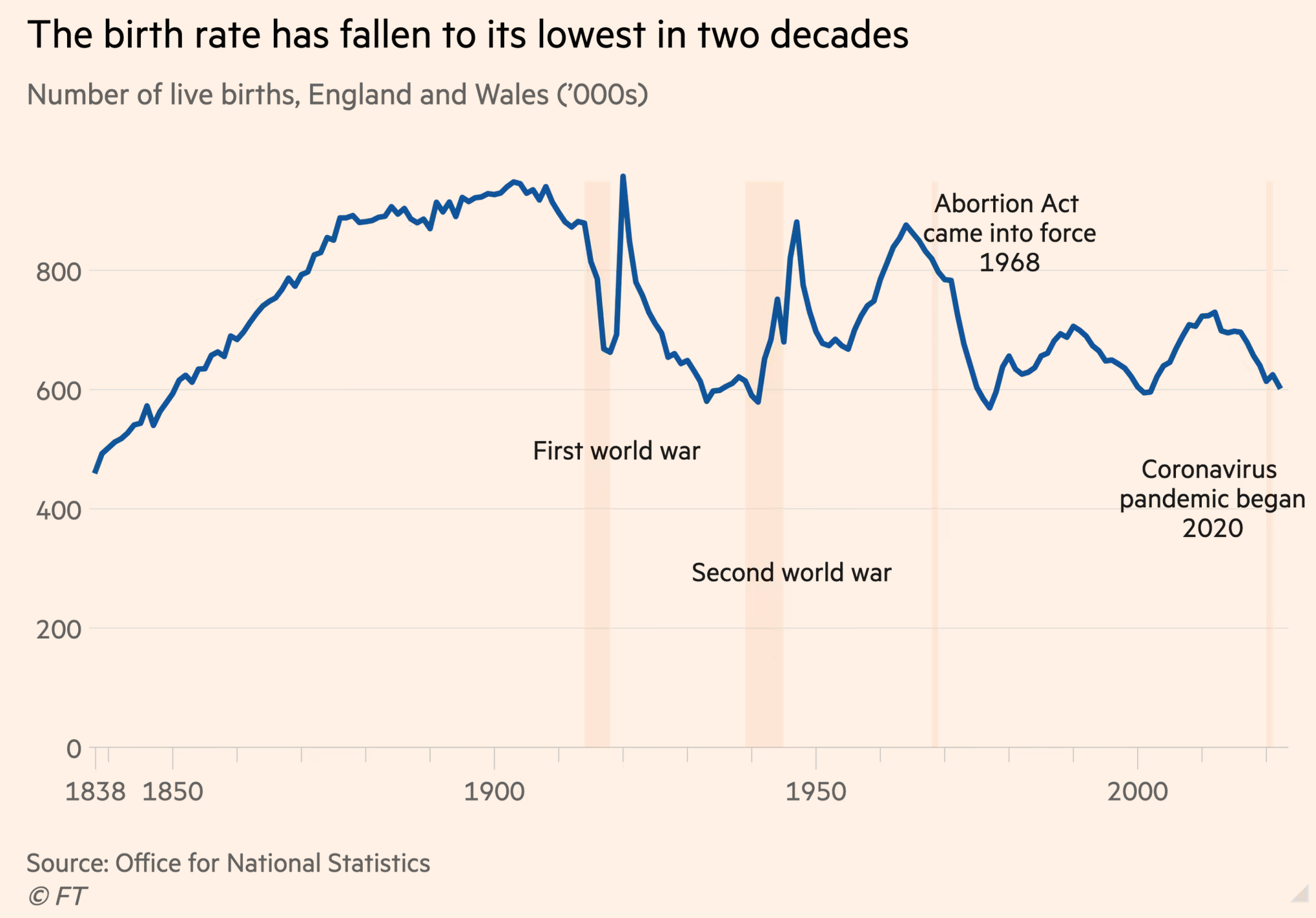
Yet, look closely. There are two very large effects of the wars ‘ending’ (baby boom started before WW2 ended). Notice that the fertility rate (here crude birth rate) actually hits the post-abortion low during the inter-war period. Curious.
Contraception availability
This is another obvious cause, namely methods for consciously preventing pregnancy. The most effective such method is the birth control pill, so here’s Denmark, which legalized the pill in 1966:
1966 is exactly the starting point for the drop to below replacement fertility levels. Just as above, however, we see that fertility almost hit replacement in the 1930s during the depression, before the post-war baby boom bought it back up to 3 children per woman briefly. This is curious because American stories of baby boom fertility are often about soldiers returning from war. Obviously, since Denmark was occupied until 1945, we had no large amount of soldiers that would be returning. In fact, if one looks closely, the fertility rate is rising during war time too, just like the British data above.
Role models and national culture
This one is harder to see empirically, but since we know that people copy role models they see around them and in the media, we know that young people are increasingly desiring to be childless due to such social contagion. And there are plenty of such high prestige, childless role models:

Some academics have tried regression models on panel data to see if they can find evidence of such social contagion among friend groups. Could say find the effect? The answer is yes (Is fertility contagious? Using panel data to disentangle mechanisms of social network influences on fertility decisions):
Using panel data (N = 1.679 married and cohabiting couples), this paper investigates the presence and causal mechanisms of social contagion processes regarding first births. Results confirmed the hypothesized positive association between the number of network members (friends, acquaintances, siblings) with young children and the respondents’ transition rate into parenthood, particularly among younger couples. Several potential intervening mechanisms underlying this social contagion effect were tested. First, evidence was found for observational learning processes in which Ego obtained information on the joys and challenges of parenthood from network members with children. Second, childless respondents tended to feel pressured from couples with children in the network to start a family. Third, results supported the notion of social opportunity costs in that the anticipated loss of social ties after becoming a parent was more likely the fewer parents there were in the network. All three mechanisms exerted a positive impact on both fertility intentions and behavior. Panel regression models relying on intraindividual change scores showed that social learning was the most robust mechanism. An additional indirect test for causality suggested that the findings were unlikely to merely reflect parental status homophily (i.e., selection effects).
I didn’t find any studies of social media or celebrity copying, but maybe such a study exists somewhere. There’s plenty of such evidence for other social behavior being copied (e.g. unusual verbal tics).
On the other hand, we have historical examples of authoritarian leaders imposing pro-natalist cultures and this seems to boost fertility rates or at least prevent further declines. For instance, Nazi Germany:

And Franco in Spain:
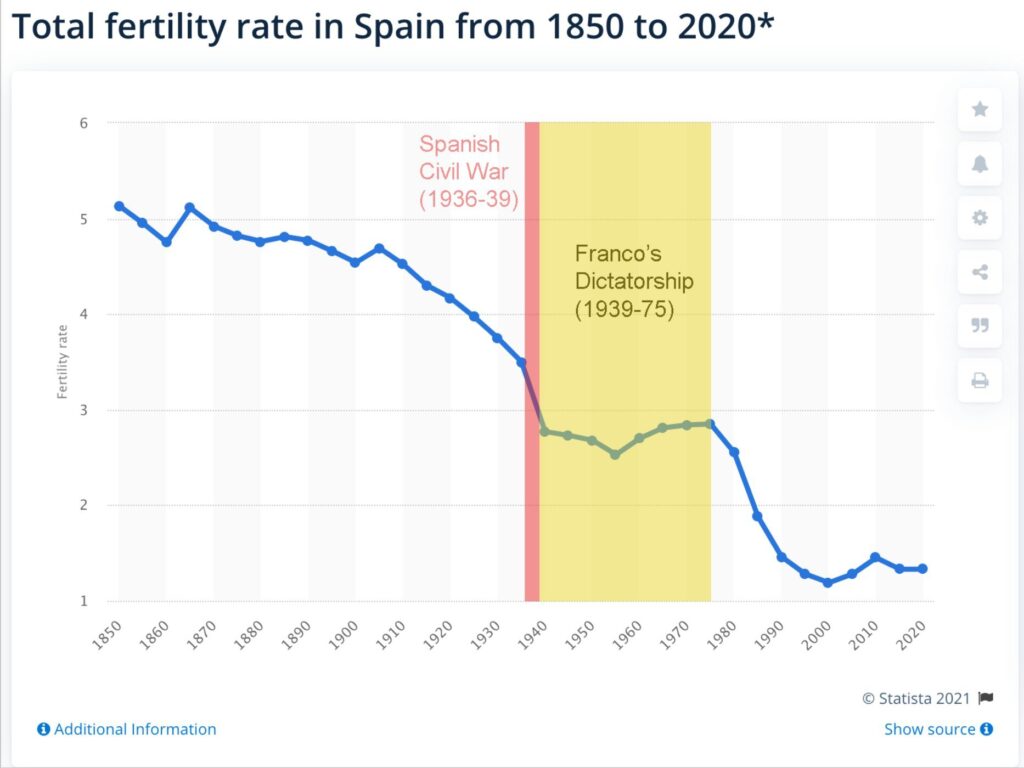
For more on this see the prior post: Authoritarianism and fertility: maybe, probably.
Disposable income cope
Before going to my final cause, I want to deal with what I think is not an important cause: money. If one does surveys of could-be parents and ask them why they don’t have (more) children, the go-to answer is that they don’t have enough money (random headline from Huff Post):
It makes intuitive sense if you don’t think for too long. Children cost a lot of money, even with socialized health care, childcare subsidization etc.
The problem is this (UK data):

The fact of the matter is that disposable income has never been higher in human history. Clearly, lack of disposable income cannot be a cause of declining fertility when it is at a historical high. Our peasant ancestors were living from harvest to harvest, and in tiny houses without proper insulation, and no flush toilets, with no AC and no radiators, and they managed to have above replacement level fertility. So I don’t think money is much of an explanation of low fertility, even if people justify it to themselves this way.
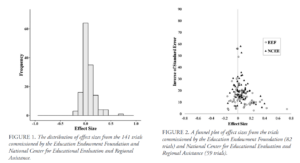
Additionally, historically speaking, the countries that got wealthiest the fastest also saw the largest fertility declines, not increases. And on top of this, policy changes to increase fertility based on economic incentives routinely fail to produce much of anything:

Notice how the larger effects are from studies with large uncertainties (publication bias).
Recent examples of right-wing countries trying to increase fertility have also not resulted in much of note. Politico has a typical left-wing attack on these:
In 2016, Poland launched its 500 plus program. Parents receive around €120 per month for every child after their first. According to the European Commission, almost 4 million children up to the age of 18 — or 55 percent of all Polish children — were covered by the program by 2017.
Results are mixed at best. Hungary’s fertility rate has increased in the past decade, from when it was lowest in the EU at a dismal 1.2 births per woman. But at the current level of 1.6, it’s still far from self-sustaining. In Poland, there was an uptick in birth rates after the introduction of the 500 plus program, possibly tied to the policy, but it soon subsided. This year the birth rate reached the lowest level since World War II.
Here’s a plot:
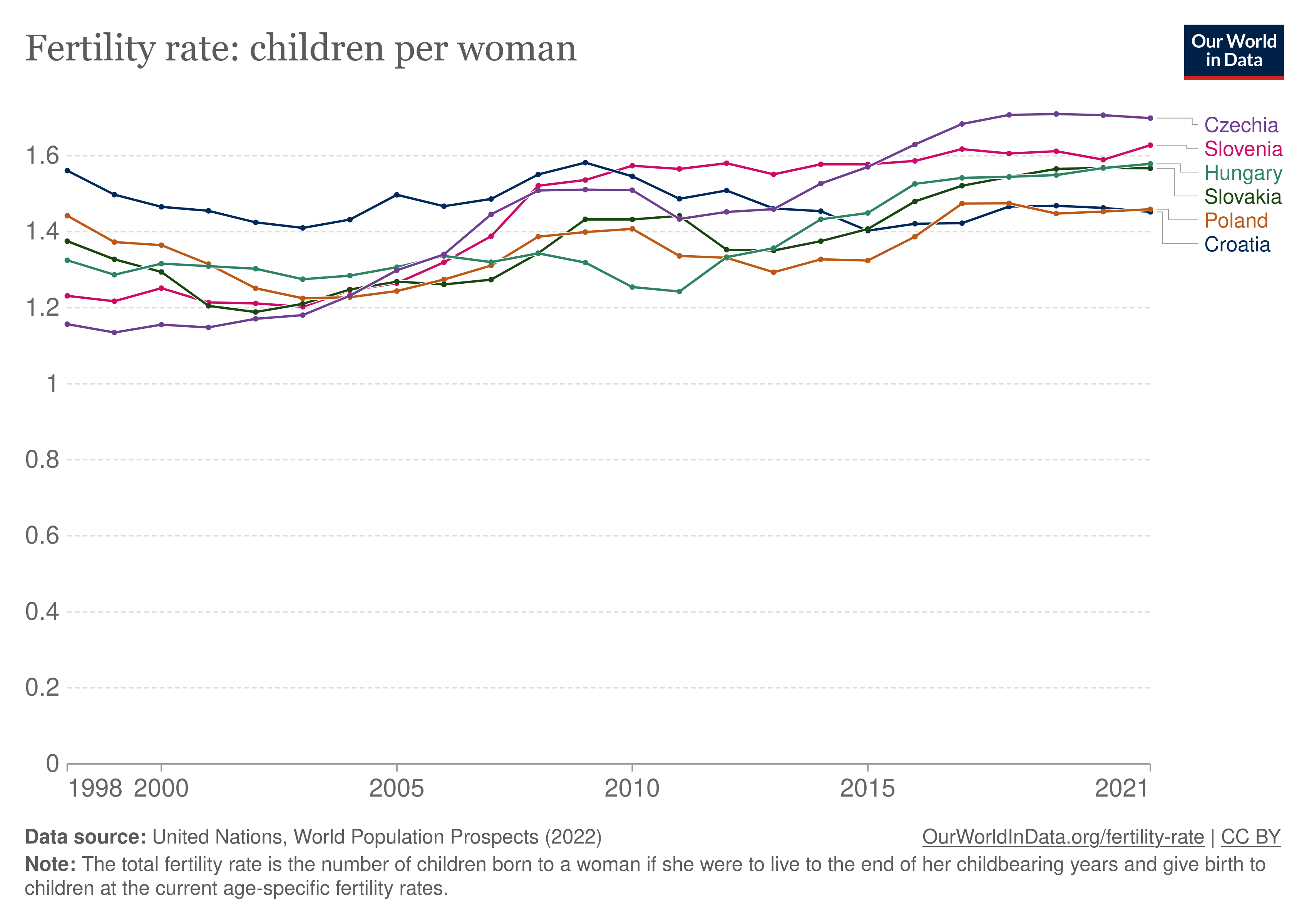
If you squint, you can see some effect. The problem is that the policy changes were made over multiple years. Hungary does show an increase in fertility since around 2010, and Wikipedia tells us that:
Several measures were introduced since 2010 that made services free or cheaper for families with children.
Vaccinations against the following diseases are free and obligatory in Hungary: tuberculosis, diphtheria, tetanus, pertussis, poliomyelitis, haemophilus influenzae, measles, mumps, rubella, hepatitis, streptococcus pneumoniae.[15] The government made vaccinations for other diseases free, chicken pox, both types of meningitis and rotavirus, in 2018.[16]
Children in the first nine years get free textbooks in school since 2017. Those in higher years but living in disadvantaged conditions, suffering from long-term illness, receiving child protection benefit, or living in a large family with three or more children are also entitled to free textbooks. However, the government plans to provide free textbooks for every pupils and students until the final exam.[17][18]
Children who live in disadvantaged conditions, suffer from long-term illness, get child protection benefit, or live in a large family with three or more children get also free or half-priced meals in nurseries, kindergartens and schools. Meanwhile, others get them on reduced prices.[19][20]
Those younger than 20 who will get a European driving license in Category B (motor vehicles) may both take a course on the KRESZ (similar to the British Highway Code) for free and try the test for the first time at no charge.[21]
For those getting a successful language exam at the B2 or the C1 level, the price of the exam is refunded by the state if the examinee is under 35 years old.[22]
Children may use public transport free if they are accompanied by an adult and do not attend school yet. Pupils, students and undergraduates may use public transport at half price by showing their student card.[23]
But other reforms were introduced in 2015 and 2018, and there’s nothing to see for them.
Poland introduced its program in 2016, which does fit with the small increase. The increase is from about 1.32 to 1.45, which is nice but not large. On the other hand, the government spending on this is massive (OECD):
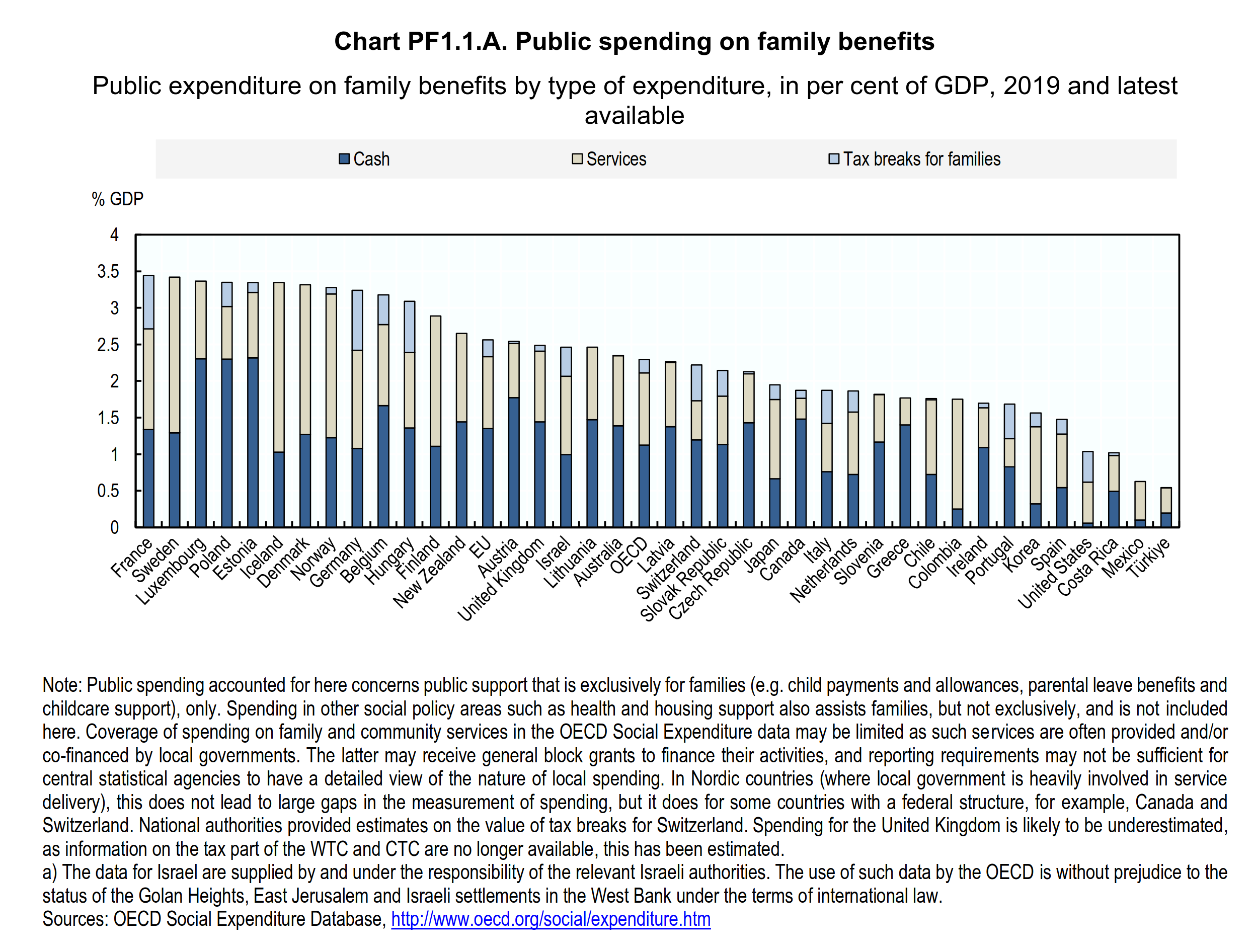
If one looks for a pattern, one can find it, sort of. Sweden has a relatively high fertility and spends a lot. South Korea spends little and has a super low fertility. Israel spends an average amount and has the highest fertility. These kinds of cross-sectional data can be very misleading. If we had broadened the sample of countries to include non-OECD countries, we would have seen a stark nonlinear pattern since the highest fertility countries don’t much of anything on family benefits (these being in Africa). This result is a misleading result of focusing on the Western countries inside which such a pattern exists.
Population density
Finally, we come to the point I want to argue since it is less commonly mentioned. There is a notion of cities being IQ shredders, since they were historically highly deadly due to infectious diseases. Here’s Greg Clark’s A farewell to Alms:
Death rates were typically much higher in towns and cities than in the countryside. Urban mortality was indeed so high that, were it not for continual migration from the countryside, the cities would have faded from the earth. In London from 1580 to 1650, for example, there were only 0.87 births for every death. Without migration the population would have declined by a half percent every year.
Early towns were generally crowded and unsanitary, so that infectious diseases such as plague, typhus, dysentery, and smallpox spread quickly. Life expectancy at birth in London in the late eighteenth century, a mere 23 years, was thus lower than for most preindustrial societies, even though London then was perhaps the richest city in the world. As late as 1800 Londoners were not able to reproduce themselves: 30 percent of all infants died in the first year of life. Indeed urban dwellers in Roman Egypt had a better life expectancy than eighteenth-century Londoners.
The greater mortality rates of towns shows in the data from the English male testators, though there we have evidence only from smaller towns such as Bury St. Edmonds, Colchester, and Ipswich and not from London itself. While life expectancy at age 25 was 56 in the countryside, it was only 50 in the towns. And while 67 percent of children born in the country survived to appear in their fathers’ wills, in the towns it was only 64 percent. Surprisingly, though, the lower reproduction rate of those in the towns was due mainly to differences in fertility. The average testator in the countryside fathered 5.1 children, while the average town dweller fathered only 4.3.
…
The data also illustrate the well-known fact that in the preindustrial era cities such as London were deadly places in which the population could not reproduce itself and had to be constantly replenished by rural migrants. Nearly 60 percent of London testators left no son. Thus the craft, merchant, legal, and administrative classes of London were constantly restocked by socially mobile recruits from the countryside.
The reason for the “IQ shredder” effect is that cities also attract above average talented people, so that historically and also in modern times, relatively bright people move to cities, reproduce less or not at all, and then die off. This is one of the causes of the dysgenic fertility pattern most countries have. Apparently, until the industrial revolution, this city dysgenic effect was too weak to counteract the positive selection for intelligence present in general, but in modern times, it is strong enough due to much higher rates of urbanization and much reduced deaths from infectious diseases.
But what is really the evidence of population density on fertility? It is possible to use longitudinal studies of countries and subnational regions to study this. There is a great paper on this that I want to highlight:
- Rotella, A., Varnum, M. E., Sng, O., & Grossmann, I. (2021). Increasing population densities predict decreasing fertility rates over time: A 174-nation investigation. American Psychologist, 76(6), 933. Ungated preprint.
Fertility rates have been declining worldwide over the past 50 years, part of a phenomenon known as “the demographic transition.” Prior work suggests that this decline is related to population density. In the present study, we draw on life history theory to examine the relationship between population density and fertility across 174 countries over 69 years (1950 to 2019). We find a robust association between density and fertility over time, both within- and between-countries. That is, increases in population density are associated with declines in fertility rates, controlling for a variety of socioeconomic, socioecological, geographic, population-based, and female empowerment variables. We also tested predictions about environmental boundary conditions. In harsher living conditions (e.g., higher homicide or pathogen rates), the effect of increased population density on fertility rates was attenuated. The density-fertility association was also moderated by religiousness and strength of social norms, where the relationship between density and fertility was attenuated in countries with high religiosity and strong social norms. We discuss why and when changes in population density may influence fertility rates and the broader implications of this work.
The estimated effect size is quite large:
Across 174 nations over 69 years of data, we found a robust association between population density and fertility, where between-country differences and within-country changes in densities over time predicted fertility rates, accounting for 31% of the variance in fertility. As population densities increased, fertility rates decreased. This pattern was observed in 116 out of 26 174 countries. These relationships were robust across a variety of analytic approaches, including different methods accounting for the potentially confounding effects of temporal autocorrelation.
And didn’t go away even with extensive controls:
Additionally, the associations between fertility rates and within-country changes and between-country differences in density, over time, were robust when controlling for a suite of socioeconomic and socioecological variables and alternative explanations for shifts in fertility: GDP, human development, inequality, homicide rates, climate stress, pathogen prevalence, population sex ratio, population relatedness, migration rates, gender inequality, access to contraception, religiosity, and tight/loose social norms. In sum, the present work provides strong evidence that declining human fertility is uniquely linked to increasing population density.
The authors discuss this from a life history perspective (what else is there?):
We posited that higher densities would lead to lower fertility rates, which we derived from life history theory. Life history theory suggests that environmental conditions with heightened ability-based social competition (i.e., predictable and stable environments with low mortality risk), people can enhance their competitive advantage by investing more resources in long-term strategies that builds their competitive ability (e.g., education). This slower strategy also entails fewer children greater parental investment. This shift in child rearing dynamics enhances long-term competitive advantage of both adults and offspring. In harsher environments where the future is less certain (i.e., higher violence, fewer resources, greater risk of mortality) there are lower payoffs for investing in long-term strategies, which favors faster competitive strategies associated with having more children, and investing fewer resources per child.
I would also add that population density makes things relatively expensive, especially the living space most needed for family formation. This makes to tough to afford housing for people living in cities, and their interest in the offerings of modernity make them really not want to move out.
The study above used the simplest measure of population density we have, namely, people/area. This is relatively easy to measure, but is also somewhat wrong. Norway has a huge area of mountains, snow, and forests in the north where almost no one lives. As a consequence, Norway has a very low population density. But in reality, most Norwegians live in a few large urban areas around Oslo, Bergen and so on. In reality, then, Norway’s population density (in some sense) isn’t that low. One could instead talk about urbanicity, as the proportion of the population living in cities. This of course just opens the question of how soon something counts as living in a city, but at least avoids the empty forests/deserts problem. If we look up a map of urbanicity, we see that Norway and Denmark have about the same values (about 85% live in cities), but the population densities are 14/km² vs. 138/km². Clearly, then, this would have been a more suitable variable to use. The authors even say they tried controlling for this variable, which seems nonsensical (controlling for the mediator or a better measure). If I had unlimited time, I would dig into their supplements which has their data and R code.
The good thing about population density (broadly speaking) is that it is something we can do something about with technology.
First, the almost availability of self-driving taxis will mean that commuting can become much cheaper and will be hands-free. Thus instead of being stuck driving a car to and from work, parents can work while going to and from work, thus cutting down on the time spent away from home. This in turn enables living further away from the job, as the time spent commuting is not just dead time for the parents. This is one of the many reasons I think promoting self-driving taxis is a good economic and demographic idea.
Second, working from home enables women (and men) to much more easily combine working lives with family making. Generally speaking, mothers with small children hate leaving them. If women could instead work from home — as they did historically — they would never have to leave them. This also entirely removes the time spent on commuting, an additional benefit. Working from home also means that people can live anywhere they like, as long as it has internet, thus reducing the urbanicity. In other words, they can get out of the cities and back to living in nice green areas. And if the costs of transport is significantly reduced by AI, then they can also relatively easily get in and out of town if they want to hang out with friends. Since the AI are driving, this can also involve drinking, and one can even sleep on the way home if one wants to.